|

Procedures
Dacryocystorhinostomy (DCR)
For patients with blocked tear duct, the usual cause of a watering eye.
|
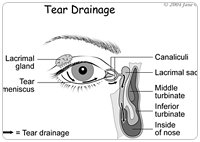
The tears normally drain from the corner of the eye close to the nose, via tiny puncta into the very fine lacrimal drainage channels (canaliculi). The tears go into the lacrimal sac, then down the nasolacrimal duct which lies in a bony canal, then opens into your nose. You are not aware of the tears draining into your nose and these go down into the throat.
The most common cause of watering eyes is a blocked nasolacrimal duct. Surgery to overcome this blockage is called "dacryocystorhinostomy" or DCR.
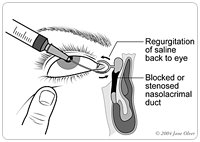
In order to confirm the site of the obstruction causing the watering, lacrimal syringing and gentle probing is done.
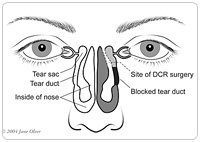
The aim of this operation is to relieve a watery, sticky eye caused by blockage of the tear duct (nasolacrimal duct) situated between the tear sac (lacrimal sac) at the corner of the eye and the tear outflow passage into the back of the nose.
DCR consists of creating a direct connection between the tear sac into the nose, bypassing the blockage and allowing tears to drain normally again. Usually some soft silicone tubes are placed, which are removed about two months after surgery.
There are two methods of doing this:
1. Externally (from the outside, via a short skin incision)
2. Internally (from inside the nose: endonasal endoscopic)
External DCR Surgery
 A small incision is made on the side of the nose to gain access to the tear sac. A little bit of bone between the tear sac and the nose is removed in order to reach the inside of the nose. The tear sac is opened and stitched to the lining of the nose so a direct passage is made between the sac and the nose. Usually a soft silicone tubing is placed from the corner of the eye , through the tear ducts into the nose temporarily to keep the passage open . These tubes are usually not noticed, are painless when in the correct position and removed between 6 and 8 weeks after the operation. Whilst the tubes are in there may be slight overflow of tears , which improves once they are removed. A small incision is made on the side of the nose to gain access to the tear sac. A little bit of bone between the tear sac and the nose is removed in order to reach the inside of the nose. The tear sac is opened and stitched to the lining of the nose so a direct passage is made between the sac and the nose. Usually a soft silicone tubing is placed from the corner of the eye , through the tear ducts into the nose temporarily to keep the passage open . These tubes are usually not noticed, are painless when in the correct position and removed between 6 and 8 weeks after the operation. Whilst the tubes are in there may be slight overflow of tears , which improves once they are removed.
|
|
The stitches are removed one week after surgery and the fine scar usually fades within three months. The tubes are removed simply in the clinic, when we look inside the nose, then divide them and retrieve them simply. An anaesthetic is not required for removal of tubes. The results are about 95% success.
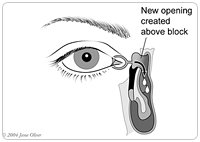
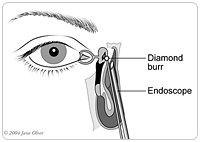
Internal DCR Surgery
In this operation -- also called endoscopic endonasal DCR -- the tear sac is approached via the inside of the nose, using a small telescopic instrument called an endoscope. This instrument allows the surgeon to visualize all the relevant structures clearly and make the opening in a similar way to above, but without placing any stitches either on the skin or inside the nose. The opening is made slightly smaller than that of the external DCR and the operation is slightly quicker. Again, temporary silicone tubes are placed and the follow up is similar to above with the tubes being removed between 6 and 8 weeks after the surgery. The results are about 86 - 90% success.
Which surgery will I have?
The external approach has a higher success rate than the internal approach. Around 90% of external DCR operations are successful. Surgical failure is due to formation of scar tissue. The disadvantage of the external approach is that there is a small skin scar on the side of the nose which is occasionally visible in some patients. The advantage of the internal approach is that it is a quicker procedure and there is no skin scar with this method. The surgical success rate of this approach is slightly less than that of the external, in a range of 80 - 85%. Both surgical approaches can be done either under general anaesthesia (patient asleep) or local anaesthesia (patient awake) where only the surgical zone is "frozen". The surgeon will recommend which type of surgery they believe is best for you.
|